Role of Electronic Apex/ Foramen Locators
Working length determination during root canal therapy has been greatly aided by Electronic apex locators (EALs). They can save time in determining initial working length, save on the number of X rays taken, and can be particularly helpful when the periapex is unclear on radiographs or when there is a question about whether a perforation has occurred. In my practice I consider it absolutely indispensable for the simple reason that foramen does not coincide with the anatomical apex in most teeth (see the pic). You can confirm this fact by examining the morphology of extracted teeth. One of the earliest brands was Root ZX by JMorita of Japan which still is the gold standard in accuracy as confirmed by various studies. I have been using it since 1993.Intraoral radiographs do not show the apical foramen and are often misleading, leading to compromising results, see below. Picture shows how radiographs can be deceptive in determing correct WL, you will never be able to assess correct WL without a good apex locator.
Determining correct WL is a critical factor in RCT success, read this excellent paper by an Endodontic giant...CLICK HERE
Once you learn about Working length, understand also what is WORKING WIDTH, this is equally important.JOE, July 1992 found in his study as follows:
Apical foramen is not at the apex in : 84% Maxillary centrals, 93% Maxillary lateral, 84% maxillary canines.
So if you are depending solely on X-rays, making an error is almost certain (If patient goes to court against you, think about it). See This
paper CLICK HERE
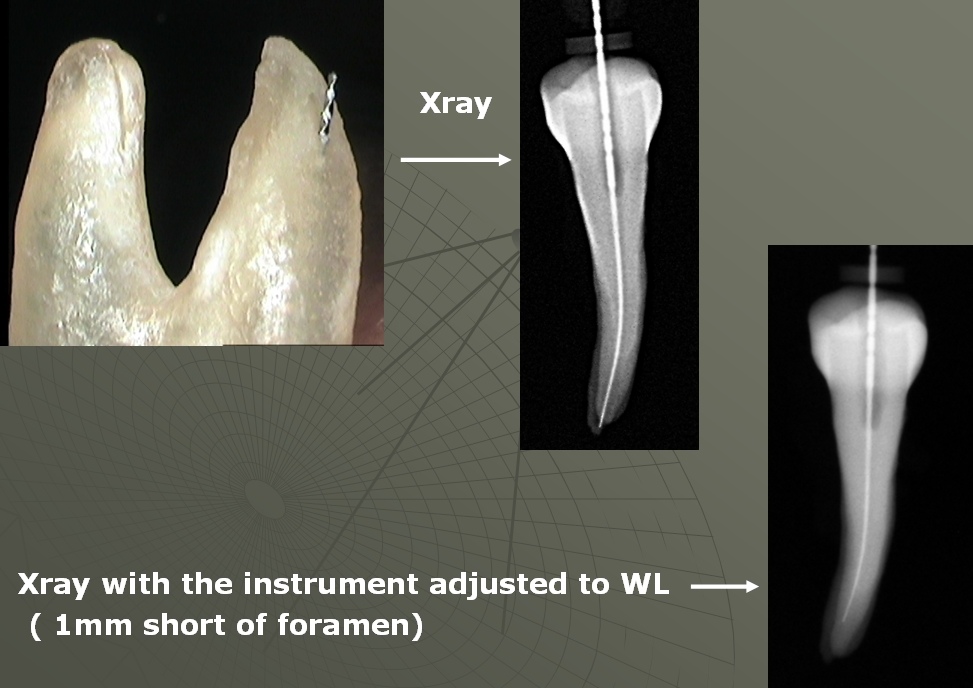
Look at the pic below, It is a mandibular first molar, how are you going to know the correct working lenght with radiograph alone ? From the point of view of science any root canal treatment done without use of apex locator is NOT Dentistry BUT Quackery. If such a patient decides to go to court I am sure will win the case.

Learn Proper Endo at one of the BEST courses, Enroll NOW
Serious about learning all about how Apex Locator works, Read this PAPER
A number of in vivo studies have shown accuracy ranging from
83-100%. EALs have gone through at least three generations of development. Early
versions used a direct current which was rather unreliable. The next generation
was improved by use of alternating currents, and the most recent EALs use
multiple alternating currents of different frequencies. Each of these changes
have made them more accurate and reliable. Two of the most popular current EALs
are the Root ZX by J. Morita, and the Apex Locator AFA (All Fluids Allowed) by
EIE/Analytic Technology.
Apex locators function by using the body to complete an electrical circuit. They measure the difference in electrical impedance (resistance to a current, in ohms) between the lip and the file in the tooth. The EAL is connected by wires to the lower lip and to a file which is placed in the root canal. The impedance between the lip and the periodontal ligament (PDL) is a known value, so as the file tip is advanced toward the PDL, the EAL detects the changing impedance values and indicates the approach to the apex on its screen.
When the PDL is contacted by the file tip, an audio alert is sounded and it is indicated visually on the screen. Since the file is contacting the PDL it is slightly past the apical constriction. This information can then be used in length determination. Like any new technology, there is a learning curve for EALs. It takes some practice to learn how to interpret the readings on the screen and develop confidence in their accuracy. Do not give up after a few tries.
Some clinicians are so confident in their use of EALs that they take only preoperative and postoperative radiographs. For most clinicians, however, it is advisable to confirm working length with a radiograph. There are several tips which are helpful in using EALs. Turn on the EAL and allow it to self- equilibrate before connecting to the patient. Be sure the file and lip clip do not contact metal restorations.
Non-conducting irrigants give the most accurate readings. These include RC Prep, alcohol or dried canals. Conducting irrigants, such as sodium hypochlorite or saline are more problematic. If a conducting irrigant is used, be certain that it doesn't allow conduction to another canal or a metal restoration. Some apex locators claim to be equally accurate with all irrigants, but clinical experience and recent literature indicates that this is not the case.
When determining working length, select a file that fits snugly at the apex. Advance it slightly past the apex and pull it back to make your readings. Do it several times to verify. If the readings are not reproducible, they probably are not accurate. Inaccurate readings sometimes occur when a periapical lesion is present.
The Root ZX apex locator was accurate for an apical size of 0.6 mm, independently of the file size; between 0.7 to 0.8 mm, we should adjust the files to the foramen, whereas above size 0.9 mm the locator is not accurate. The results show that the accuracy of this electronic apex locator is gradually lost as the foramen widens. Considering the stable conditions of in vitro studies, our findings advise caution in clinical application of the locator. (J Endod 2011;37:1306–1309)
The position of the file tip on an x-ray is always somewhat suspect, as the relative position of the file does not tell the clinician where the Minor Constriction of the apical foramen is in relation, only how far the file tip is from the radiographic terminus. It must be remembered that the apical foramen can exit the tooth from the anatomic apex and up to 4mm from the radiographic terminus. This huge variance can lead to a significant deviation in interpretation with regard to the position of the Minor Constriction. As an aside, interpretation of the position of the file and its significance at the root end is similar in its limitations as looking at a single x-ray of a root canal treated tooth and evaluating whether the apical filling is really placed to the Minor Constriction. Developmental errors in x-ray processing can also lead to difficulty reading radiographs as can only relying on a limited number of views. (by Rich Mounce)
Also see this CLICK HERE to read how apex locator helps in finding perforation
Tweet