Marketing forces in Rotary Endodontics
Endodontics forms a good volume of practice for general dentists. As dentists when we proclaim ourselves as part of scientific community, it is our duty to base our treatments on science rather than convenience or give in to the lure of marketing.
In a Sept-Oct 2007 issue of General dent. an article by Francis W. Allen points out that 20% apical cleaning was possible with hand instruments, with the use of Tapered instruments you are able to clean only 18% in the apical 1mm, no wonder we spend so much energy on retreatment, to read the full paper CLICK HERE
We routinely resort to apicoectomy when endo treatment has failed, I wonder why should it be hard to understand that cleaning/disinfecting apical area is most crucial for root canal success.
It should be the responsibility of the opinion leaders/Endodontists to disseminate true scientific facts, for general dentists to follow. Are we being sold out to commercial interests? CLICK HERE to See Cliff Ruddle's paper and response. Almost all talks and courses are sponsored by big companies. Should that prevent us from telling the truth? In a recent course on a popular tapered rotary system, one participant asked, “Sir I am also following this tech for the past 7 years, still my radiographs do not look like yours”. The speaker privately confided that he uses another system for apical preparation (LSX).
Protaper and Profile vortex transport apical foramen (All tapered would do the same)
We know the size of the taper is one of the main factors involved in apical root transportation because an increase in the taper reduces instrument flexibility. Apical transportation promotes the harbouring of debris and residual microorganisms as a result of insufficient cleaning of the root canals.
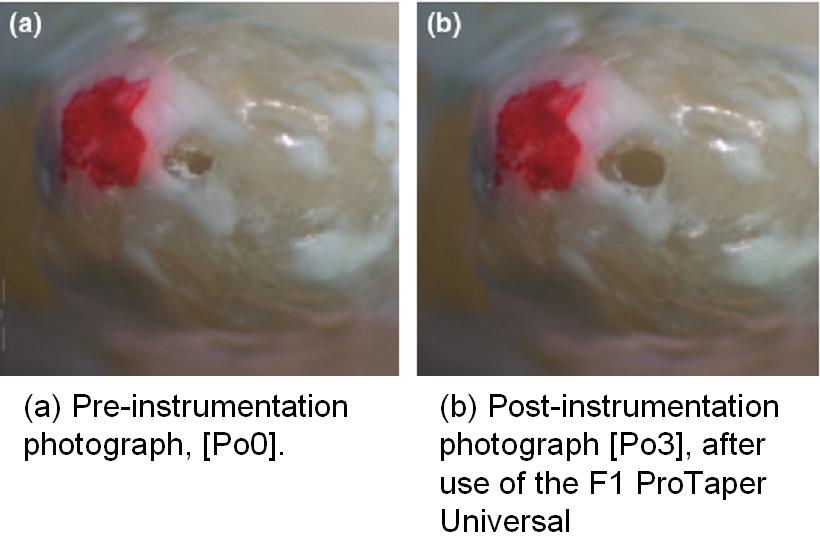
NOW this study clearly demonstrates in most samples, the ProTaper Universal and ProFile Vortex files produced transportation of the major foramen and created an oval-shaped major foramen after over instrumentation. See fig, FULL PAPER
General dentists try to follow the advice of the speakers, and when they do not succeed as described in courses they try various “tricks”. Read on…..
Recently I came across two interesting observations, one colleague told me that the prognosis for root canal treatments is better if after the biomechanical preparation, the canal is flooded with sodium hypochlorite and the ultrasonic scaler tip is vibrated in the pulp chamber for five minutes.
I almost gasped when another colleague told that he uses 5% sodium hypochlorite with his tapered NiTi rotary system, without using rubber dam. On close questioning I learned that the sodium hypochlorite is not used for irrigation, but the rotary instruments are just dipped into the solution before inserting into the canal. He didn’t think it made much difference if no irrigation is done, because the rotation of the instruments will bring all debris to the coronal portion!
Coronal flaring is one step that has made a great difference in root canal treatment. But are we overdoing it ? Because of large taper instruments you need to make coronal access wider, these instruments (tapered) also cut too much in the furcation area causing strip perforations. Weakening of coronal and furcation area makes tooth highly vulnerable to fracture (this is the area which undergoes flexure during function- Abfraction) . It is hilarious to see tapered school making fuss about excess apical dentine removal.
With concentrating more on greater and greater coronal flare, proper enlargement and thus cleaning of the apical portion is being overlooked. Any one who has taken a look at the literature will have no doubt that the apical enlargement has to start from #30 instrument, not stop at #30. But with information being circulated like ‘In an untreated tooth, the diameter of the foramen is normally between 15 and 20 hundredths of a millimeter’, when no experienced academicians oppose such loose statements, how can one blame busy clinicians for not properly cleaning the apex?
Another dentists called the other day and he described his technique as:...
- I first establish glide path using 10 no k file .
- Then according to the length it has entered the canal i enlarge the orifice to 20 k file
- Then i use GG drills 1-4 to enlarge the orifice .
- Then i use hand files to enlarge the apex till file 25
- then i use profile 06 25 to working length of the canal .
- then enlarge the apex using file 30-35 or 40 to finish the case .
And he said he uses lateral condensation for obturation, it is so exhausting becos I have to put so many cones to fill and achieve proper fill.
It pains to see the kind of misinformation that is creating a mess in the minds of these dentists and leading to suffering for them and their patients. Call for a course today.
Tweet